Maternal Mortality and Morbidity



 +3
+3Kelly Lavin, PhD & 6 others
August 22, 2021

The United States’ maternal mortality rates, in 2018, were 17.4 deaths per 100,000 births, the highest among developed countries (CDC, 2018; Tikkanen et al., 2020). Addressing these alarming rates, the CDC launched the Hear Her Campaign, which aims to save mothers’ lives by 1) raising awareness of warning signs and the potential for illness/loss of life, 2) sharing resources, 3) reducing stigma and sharing of moms’ experiences, and 4) educating providers on interventions. Hear Her created key resources to foster conversations regarding maternal health among women, families, and providers (Figure 1; CDC, 2021).
This article extends the work of the Hear Her Campaign by discussing the prevalent maternal mental health concerns and demonstrating how Colorado has integrated public health messages and health care system coordination to actualize the goals of the Campaign.
Figure 1
CDC’s Hear Her Campaign’s Urgent Maternal Warning Signs Poster
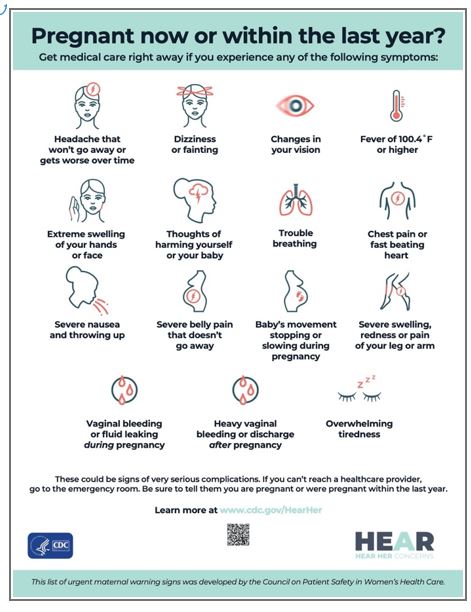
Note. For access to additional resources and resources in other languages, please visit: https://www.cdc.gov/hearher/resources/posters-handouts.html#urgent
Perinatal mental health disorders are common. Depression, post-traumatic stress disorder, and anxiety-related disorders (including generalized anxiety disorder, obsessive compulsive disorder, panic disorder) show elevated rates around birth and have associations to adverse birth outcomes, as well as maternal and infant mortality (Howard & Khalifeh, 2020). Approximately 10-20% of women experience depression across the perinatal period and one in five women experience anxiety-related disorders around the delivery period (Tikkanen et al., 2020; Fawcett et al., 2019).Perinatal mental health also encompasses comorbidities such as substance use and intimate partner violence, which are critical to integrate for appropriate treatment (Shen et al., 2020; Van Niel & Payne, 2020).
While most research focuses on pregnancy through one year postpartum, the perinatal period and increased risk for mental health concerns extends beyond the time of birth. Perinatal best encompasses all phases of pregnancy (e.g., fertility issues, miscarriage and other fetal losses) through age 5-years-old or later (Moyer & Kinser, 2021). Elevated and new onset perinatal mental health issues vary widely, with some experiencing symptoms during pregnancy and/or years after delivery (Lomonaco-Haycraft et al., 2018). Because perinatal mental health concerns affect parenting partners and siblings in addition to mothers, it is important to acknowledge the scope of people affected. Perinatal mental health concerns are found to occur at comparable rates in mothers and fathers and while sparsely studied, perinatal disorders and losses are presumed to impact older siblings (CDC, n.d.; Paulson & Bazemore, 2010; Scarff, 2019; Gjerde et al., 2020; O’Leary & Gaziano, 2011).
Perinatal mental health rates highlight racial and ethnic health disparities. Rates of postpartum depression is higher for mothers self-identified as Black, Latinx, American Indian/Alaskan Native, and Asian/Pacific Islander (Ko et al., 2017). Despite these evident disparities, women of color are less likely to be screened for depression during the postpartum period relative to White counterparts (Sidebottom, 2021). Data also shows further exacerbated perinatal mental health rates during the COVID-19 Pandemic, particularly for low-income and diverse communities, which also face a lack of professional and perinatal/infant and early childhood mental health trained providers (Farrell et al., 2020; Osborne et al., 2020; Wadsworth et al., 2018; Gur et al., 2020; Masters et al., 2020; McKnight-Eily et al., 2021; Colorado Health Institute, 2020; Perigee Fund, 2020).
Awareness of symptoms, risk factors, and cascading impacts of the perinatal mental health disorders is critical for prevention and early intervention. Detailed reviews of the phenomena of perinatal mental health disorders and interventions are beyond the scope of this article but readily available (Lomonaco-Haycraft et al., 2018; Myors et al., 2013). Table 1 and Figure 2 includes examples of common perinatal mental health symptoms and risk factors. Intervention resources are also provided below.
Table 1
Common Perinatal Mental Health Concerns and Associated Symptoms
| Mental Health Concerns | Symptoms |
| Depression | Guilt, shame, or self-blame; difficulty bonding with baby; detachment from social support; believing “I am a bad mother,” “I’ve made a mistake” |
| Generalized Anxiety Disorder | Hypervigilance and insomnia; irritability; hyper-focus on control over baby’s schedule, feeding, or other aspects of baby’s care |
| Obsessive Compulsive Disorder | Intrusive, recurrent thoughts about harming self or the baby |
| Post-Traumatic Stress Disorder | Avoiding medical appointments or other anxiety-related situations; hypervigilance and insomnia; irritability; distressing dreams |
Figure 2
Common Risk Factors of Perinatal Mental Health Concerns

Given the high prevalence, it is important to raise awareness of perinatal mental health concerns co-occurring with and beyond depression. Awareness campaigns and public health interventions often do not represent the diversity in communities. Targeted messaging about perinatal mental health is, typically, devoid of the experiences of women and birthing people of color, which contributes and perpetuates inequities, leaving these families to struggle with a sense of isolation about these disorders (Taylor & Gamble, 2017). The Hear Her Campaign aims to raise awareness of these disparities and highlights stories from women of color. To best support and advocate for communities of color, it remains critical to continue to implement public health interventions and campaigns with an equity and justice lens.
For example, the Colorado Department of Public Health and Environment (CDPHE), launched the Pregnancy-Related Depression and Anxiety Public Awareness Campaign highlighting depression and anxiety, as well as support resources to families. For more information, please visit: https://cdphe.colorado.gov/pregnancy/pregnancy-related-depression
Examples of Specialized Perinatal Mental Health Interventions
To complement the anti-stigma and awareness campaigns of Hear Her and state efforts such as the link above from CDPHE, next we share some local perinatal-specific mental health interventions to dovetail the information delivery efforts.
The Caring for yoU and Baby (CUB) Clinic. The CUB Clinic integrates a range of mental-health service delivery with workforce development efforts by training advanced level graduate students in Perinatal to Five (P-5) specific interventions delivered in person or via telehealth in English and Spanish. The CUB Clinic strives to recruit and retain clinicians of color and bilingual, bicultural Spanish-speaking clinicians to serve our large and growing Latinx population. CUB strives to keep services either free or at low-cost to families by funding service delivery through Medicaid insurance billing and cultivation grant funding. Some CUB specialized services include: (1) Parentline Colorado, which is a free brief strategic psychotherapy in English and Spanish through video or telephone (2) perinatal parent support groups online in English and Spanish based on Group Interpersonal Psychotherapy to ease anxiety, promote community, and bolster social support, and (3) the WePlay Program, which is a weekly parent-infant/toddler play and social support group facilitated by the CUB Clinic and the Children’s Museum of Denver at Marsico Campus (Scarff, 2019). For more information regarding additional CUB Clinic services, please visit https://psychology.du.edu/clinics/cub-clinic.
Below are Some Additional Mental Health Resources
The Colorado Chapter within the Postpartum Support International (PSI) Network provides resources for P-5 families across the state. More information regarding resources may be found here: https://psichapters.com/co/
The Colorado Maternal Mental Health Collaborative also aims to support P-5 families through the initiative Parents Thrive. Resources for families may be accessed through this link: https://parentsthrive.org/resources/
Summary
We must do even better. Critical campaigns such as Hear Her are far from enough. Extensions of resource allocation, public awareness efforts, coordinated provision of health care and investments in research are essential but nearly absent in inclusion of all parents and parenting partners (e.g., fathers, LGBTQ+, and adoptive parents). Relative neglect of these parents exists despite well documented impacts of perinatal mental health problems on fathers’ functioning and, in turn, the growth and development of their children (Ramluggun et al., 2020). Similar devastating patterns are emerging in research with lesbian co-partner, adoptive parents and likely present for many other co-parents (Maccio & Pangburn, 2012; Foli & Gibson, 2011; Darwin et al., 2021). More applied clinical research with an equity lens is needed to support the well-being and positive outcomes of our most vulnerable communities.